Around the world, Christian organizations provide a significant portion of health care services, helping to protect and maintain the health of community members in underserved populations. To create a better understanding of the nature, scope and location of Christian health assets in low- and middle-income countries, CHA and five other founding organizations are working in collaboration to help accurately reflect this data. Together, through the recently established Christian Health Asset Mapping Consortium (CHAMC), the alliance seeks to develop a metadata platform (or "database of databases") that can be used and shared publicly; to disseminate information around Christian health services; and to evaluate current resources on Christian health assets to improve their access so that stakeholders — and decision-making around policies — can be better informed.
1
In this column, Carolyn O'Brien, program advisor at Christian Connections for International Health, a founding organization of the Christian Health Asset Mapping Consortium, and Dr. Samone Franzese, family medicine physician with the U.S. Army and Johns
Hopkins Master of Public Health candidate, where she became involved in this work, outline the consortium's unique position in emphasizing the importance of the quality, reporting and sharing of all types of health assets in the Christian health landscape,
not just those services provided in facilities and hospitals.
Having a more comprehensive understanding of these faith-based health care assets will assist health leaders and funders as they address the limitations and gaps in local, regional, national and global health systems. This understanding will also enable
faith-based health providers to more appropriately highlight their strengths and better serve their communities.
UNCOVERING THE BREADTH OF THE CHRISTIAN HEALTH ASSET LANDSCAPE
SAMONE FRANZESE, MD, and CAROLYN O'BRIEN, MSPH
The Christian Health Asset Mapping Consortium was established in 2022 with the objective of gaining a deeper insight into the capabilities, limitations and roles of faith-based organizations in low- and middle-income countries. The consortium's six founding
organizations, aside from CHA and Christian Connections for International Health, include the Africa Christian Health Associations Platform, International Christian Medical and Dental Association, The Dalton Foundation and the World Council of Churches.
By quantifying health care services, the alliance aims to enhance the understanding of the operations and infrastructure of Christian health assets and services and to foster the collaboration, learning and sharing of its resources in low- and middle-income
countries.
What are the elements of the Christian health landscape?
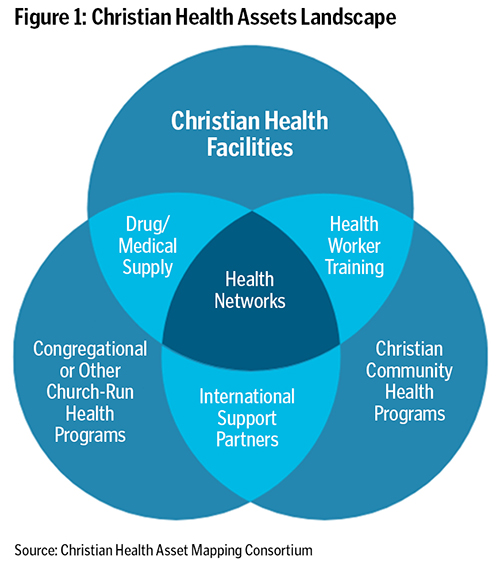
Faith-based organizations deliver health care services through various channels, such as faith-owned health facilities, congregations, community-based organizations and national and international organizations.2 These services cover a wide
range of areas, including clinical care at different levels, preventive care like immunization campaigns and cancer screenings, facilities for older adults, early diagnosis and treatment for Hansen's disease, HIV/AIDS education, maternal and newborn
care, emergency care, family planning services and more. Faith-based organizations also operate training institutions to educate health care workers and allied professionals. A unique aspect of this initiative is that the Christian Health Asset Mapping
Consortium focuses on documenting all types of health assets within the Christian health landscape, including those that are not easy to quantify, such as community health programs. Figure 1 on this page illustrates the elements of this landscape.
What do we know about Christian health care services already?
Given their remote locations, long-term commitments, influential roles in communities, and ability to reach and connect with hard-to-reach populations, faith-based organizations are positioned to continue playing a substantial role and making a profound
impact through their provision of health care services in low- and middle-income countries. For instance, faith-based organizations often operate in underserved areas and sometimes are the only point of entry for rural populations.3 However,
determining the proportion of health services they provide is challenging, as it varies considerably from urban to rural areas. In sub-Saharan Africa, this proportion can be much higher in rural areas where faith-based organizations sometimes run
the only available hospital or clinic.4 Additionally, they are frequently deeply rooted in the communities they serve, allowing them to implement interventions that consider local customs and culture. Moreover, religious actors, such as
Catholic leaders, have influential voices in their communities and help promote health and wellness in such areas as vaccine education and family planning services.5
What limits our understanding of Catholic health care's global reach and impact specifically?
While the Vatican tracks the estimated number of Catholic hospitals and dispensaries around the world, there is not a centralized resource to find clinics, community health centers and the number of community health programs — among other metrics
— that are provided by Catholic health organizations.6 It is important to not only comprehend the extent of Catholic health organizations' secondary and tertiary level services, but also the number and location of community-based
health programs, preventive services, health worker training institutions and the status of supply chains that serve them.
Although Catholic health organizations are estimated to account for 26% of health care services globally,7 it is uncertain whether this captures Catholic health assets that are integrated into other types of faith-based or public health networks.
Christian denominational plurality — which is misunderstood by many outside church communities — introduces another layer of complexity to health asset mapping efforts, especially given the centuries-long divisions and fragmentation of
various denominations.
Apart from a centralized location to access services provided by faith-based organizations, there is a need for a unified method to quantify the care provided. The analysis is inconsistent, as there is no clear distinction between the types of service
offered, its rural or urban locations, the organizational structure of each location and how to access these services. This lack of understanding was further exposed at the onset of the COVID-19 pandemic, when responses from health systems were fragmented.
Additionally, the number of faith-based health care facilities is dynamic, with facilities closing and opening daily around the world.
Understanding the limitations and gaps in faith-based health care services will enable us to address them and ultimately strengthen health systems. Faith-based organizations serve a significant proportion of the population in many countries and should
have a say in health system governance and decision-making that promotes self-sustainability and collaboration. However, to advocate for their participation, we must clearly demonstrate the impact that they make.
How is the consortium taking this work forward?
At its launch, CHAMC established three initial objectives. First, it aims to develop a metadata platform accessible to organizations and individuals to enhance their understanding of known data sets. Second, it seeks to disseminate information about Christian
health services by providing summary reports and databases to inform stakeholders and policies. And third, CHAMC aims to evaluate current available resources on Christian health assets and develop plans to improve how members can access these resources.
In working towards its objectives, the consortium published a data brief in April 2022 that examined the scale of Christian health services in 15 sub-Saharan African countries, identifying more than 8,000 health assets, including national-level hospitals
and community-level programs.8 Although this is a promising starting point, the report acknowledges that some health assets were not captured, and the scale and scope of health assets in the remaining countries of the continent must be
documented.
By quantifying Christian health care services in low- and middle-income countries, the consortium hopes to better understand where and how Christian health assets operate within their diverse and dynamic contexts and systems. This initiative is critical
in showing the impact of faith-based organizations and advocating for their seat at the table for health system governance and collaborative decision-making with local leaders and partners.
If you or your organization are interested in engaging with the Christian Health Asset Mapping Consortium, please reach out to mapping.
[email protected].
CAROLYN O'BRIEN serves as program advisor for Christian Connections for International Health, where she manages its efforts on the Christian Health Asset Mapping Consortium and supports the organization's global health programs. DR. SAMONE FRANZESE is a family medicine physician in the U.S. Army, currently stationed at Madigan Army Medical Center at Joint Base Lewis-McChord in Washington. She is a Master of Public Health candidate at Johns Hopkins Bloomberg School of Public Health.
NOTES
- "Christian Health Asset Mapping Consortium," Christian Connections for International Health, https://www.ccih.org/christian-health-asset-mapping-consortium/.
- Jill Olivier et al., "Understanding the Roles of Faith-Based Health-Care Providers in Africa: Review of the Evidence with a Focus on Magnitude, Reach, Cost, and Satisfaction," The Lancet 386, no. 10005 (October 31, 2015): 1765-75, https://doi.org/10.1016/S0140-6736(15)60251-3.
- Phesheya Ndumiso Vilakati et al., "The Neglected Role of Faith-Based Organizations in Prevention and Control of COVID-19 in Africa," Transactions of The Royal Society of Tropical Medicine & Hygiene 114, no. 10 (October 2020): 784–786,
https://doi.org/10.1093/trstmh/traa073.
- Barbara Schmid et al., "The Contribution of Religious Entities to Health in Sub-Saharan Africa," African Religious Health Assets Programme, 2008, https://www.researchgate.net/publication/237090449.
- Allison Ruark et al., "Increasing Family Planning Access in Kenya through Engagement of Faith-Based Health Facilities, Religious Leaders, and Community Health Volunteers," Global Health: Science and Practice 7, no. 3 (September 2019): 478-490,
https://doi.org/10.9745/GHSP-D-19-00107.
- "Catholic Health Care," GoodLands, https://catholic-geo-hub-cgisc.hub.arcgis.com/pages/catholic-healthcare.
- "Catholic Health Care."
- "Summary Report from 16 Africa Christian Health Association Platform Members," Christian Health Asset Mapping Consortium, April 2022, http://ccih.org/wp-content/uploads/2022/05/ACHAP-Member-Data-Summary-April-2022_final_final.pdf.